
More Data on the Low-FODMAP Diet
“This idea of IBS being just in a patient’s head is not true, and it clearly needs to be thought of as somewhat of a potentially infectious disease, at least in a sizable composite of patients. We can do better with dietary treatment.”
 A randomized controlled trial from the University of Michigan looked at a low-FODMAP diet versus a control diet (based on modified National Institute for Health and Care Excellence (NICE) guidelines). Both studies were administered by dietitians, among participants with diarrhea-predominant IBS.[1] What they found was that the low-FODMAP diet made a tremendous difference in regard to the symptom-based composite endpoint used in this trial and in quality of life.
A randomized controlled trial from the University of Michigan looked at a low-FODMAP diet versus a control diet (based on modified National Institute for Health and Care Excellence (NICE) guidelines). Both studies were administered by dietitians, among participants with diarrhea-predominant IBS.[1] What they found was that the low-FODMAP diet made a tremendous difference in regard to the symptom-based composite endpoint used in this trial and in quality of life.
This same research group took evaluation of the low-FODMAP diet a step further. They looked at the effect of the low-FODMAP diet on visceral nociception (the sensory nervous system’s response to certain harmful or potentially harmful stimuli) by changing the gut microbiome.
“It makes sense that if you have this fermentable sugar going into the gut where there is potential for fermentation by bacteria, there may be changes in that gut bacteria, such as selective up regulation of some bacteria and down regulation of others. They actually showed that there are changes in the gut bacteria, which reflected changes in intestinal permeability.”
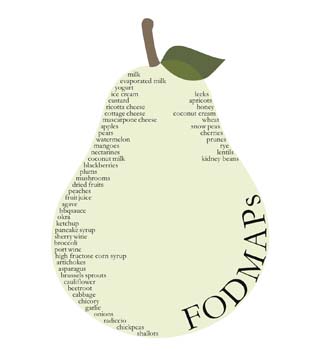
Presented at the Digestive Disease Week 2016, the study focused on the fermentable oligo-, di-, and mono-saccharides and polyols (FODMAP) diet. This diet is used in irritable bowel syndrome (IBS) and is something that continues to be very effective from a gastroenterologist perspective.
Conclusion
Primary care givers were advised that when treating IBS patients, a diet that includes low amounts of fermentable types of carbohydrates, which the colonic and distal small bowel actually can ferment, causing a lot of different pain and sensory symptoms. Getting a dietitian involved can make a big difference, especially if these patients aren’t seeing a gastroenterologist and are managed in primary care; however, gastroenterologists should also be involving a dietitian to counsel their patients.
(1) https://www.todaysdietitian.com/newarchives/072710p30.shtml












